
The largest organ in the body is the liver, an indication of its importance in health. It is involved with almost all of the biochemical pathways that allow growth, fight disease, supply nutrients, provide energy, and aid reproduction. Liver cells, which are called hepatocytes, go through thousands of chemical reactions every second in order to perform these myriad functions. Since the liver is involved with almost all biochemical processes it is no wonder that there are many different diseases that will affect it. This page will cover some of the more important ones we see in animals.
Even though it makes for good reading, you can skip the anatomy and physiology section and go right to the section on specific diseases if that is all that interests you:
- Infectious canine Hepatitis
- Liver Shunt
- Hepatic Lipidosis
- Cancer
- Chronic active Hepatitis
- Copper Storage Disease
The word “hepatitis” will be used throughout his page. Hepatitis is a general term meaning inflammation of the liver. There are many diseases that cause this, some of them are much different that what we encounter in homo sapiens.
Anatomy
The liver is a multi-lobed organ that is located at the most forward part of the abdomen. It is so far forward that it lays up against the diaphragm, the muscle that aids in breathing in mammals (birds and reptiles do not have a diaphragm).
This autopsy picture of a cat shows the gallbladder in green, with several lobes of the liver laying right up against the diaphragm (towards the top of the picture). On the other side of the diaphragm is the chest cavity containing the lungs and heart.

This close-up of the gallbladder and one of the lobes of the liver gives you a feel for what a normal liver lobe looks like in a cat.

The gallbladder can be seen with ultrasound

The liver is the largest organ that is located in the body, a testament to its importance. It has 6 distinct lobes organized into 3 regions. Like the kidneys, 25% of the blood ejected with each beat of the heart goes to the liver. Of tremendous significance is the fact that a healthy liver has great reserve power, using only a small amount of its full potential at any one time. Unfortunately, this great reserve power means that diseases that affect the liver can be well entrenched before a diagnosis is made. This obviously makes the prognosis worse. The liver does have an advantage though. Liver cells (hepatocytes) can regenerate themselves. This regenerative ability allows a diseased liver to return to normal function in some cases. Very few organs in the body have this ability.
The liver is supplied with nutrients from the hepatic artery and the portal vein, which is different from other internal organs.
The extensive blood supply to the liver is apparent in this picture.

Biliary System
The biliary system consists of the gallbladder, bile ductules, hepatic ducts, and the common bile duct.
The gallbladder is located between two of the liver lobes. It stores bile that is made by the liver, and secretes this bile through the common bile duct into the beginning of the small intestine (duodenum). The bile that is secreted into the duodenum aids in the digestion of many compounds, especially fat.
This is a picture of a greatly enlarged gall bladder and common bile duct in a cat.
BD- Bile duct
GB- Gall Bladder
L- Liver

The bile that is stored in the gallbladder is secreted into the beginning of the small intestines (called the duodenum) through the common bile duct. This picture gives you a great view of bile as it is being secreted.

Physiology
It is an understatement to say that the liver is an important organ. Its complexity precludes us from discussing all of its functions, so we will limit the physiology section to some of its more important functions.
The liver has reserve functional power and can operate effectively when most of the hepatocytes are not working well. In addition, diseased hepatocytes can actually regenerate and return to normal function.
Metabolism
The liver is the organ that orchestrates the metabolism of fats, carbohydrates, and protein. It does this in conjunction with the circulatory system, the lymphatic system, and the endocrine (hormone) system. A healthy liver is critical to proper protein, carbohydrate, and fat metabolism.
Detoxification
Drug detoxification is an important liver function. It is a complex process that occurs in the endoplasmic reticulum of the hepatocyte. Several phases are involved with this detoxification:
Bile Metabolism
Bile is made up of electrolytes, cholesterol, bile acids, bilirubin, and globulins. It is produced by hepatocytes, secreted by hepatocytes into channels in the liver called bile cannaliculi, and stored in the gall bladder Drugs are eliminated in the bile, red blood cell are recirculated through the bile system, and fats are absorbed from the intestines into the bloodstream only in the presence of bile.
The fat soluble vitamins, A, D, E, and K, require bile for proper absorption form the intestines. These vitamins are stored in the liver, and are converted to active compounds as the liver maintains normal physiology (homeostasis).
Coagulation Factors
The proteins that initiate and maintain clotting of blood are synthesized by the liver. These proteins go through very complex biochemical processes to achieved this vital function. A diseased liver is unable to synthesize these proteins, leading to a potential bleeding problem. Vitamin K is also an essential component of these clotting mechanisms. When rat poison (warfarin poisoning) is ingested it interferes with the ability of vitamin K to perform this vital function.
Red Blood Cell System
The liver removes old or damaged red blood cells from the circulation, and is involved with the storage of iron and the breakdown of hemoglobin. Because of this, chronic liver disease could cause anemia. The liver (along with the spleen), is a storage organ for blood. If these is a severe blood loss the liver expels this blood into the bloodstream to help make up for the loss.
Reticuloendothelial System
Specific cells called Kupffer cells line the inside of the liver. These cells are part of the immune system. They eliminate and degrade the substances that are brought into the liver by the portal vein. Some of these substances are bacteria, toxins, nutrients, and chemicals. A diseased liver will not filter these compounds normally, resulting in toxic accumulations of toxins, chemicals, or bacteria. Excess accumulation of bacteria in the bloodstream is called septicemia, and is one of the reasons that antibiotics are commonly used in liver disease.
Vitamins
Many vitamins are stored in the liver, and perform their functions only when activated by the liver, and are degraded by the liver. These include some of the B vitamins and Vitamin C, along with A, D, E, and K previously described.
Cause
Trauma
Animals that receive a severe and blunt blow to the front of the abdomen can suffer from liver disease. The most common cause of this type of blow is being hit by a car. A liver lobe can be fractured and bleed into the abdomen, even leading to death. A more common occurrence is a bruise (contusion) that heals itself. Heatstroke, diaphragmatic hernia and liver lobe torsion can also cause liver problems.
Inflammation
An inflamed liver is called hepatitis. Trauma can cause this, along with drugs, bacteria, bile, and toxins.
Pancreatitis
The severe inflammatory process that occurs with digestive enzymes can spill over into the liver and cause severe disease.
Anemia
Hemolytic anemia can decrease the oxygen available to liver cells and lead to their death.
Infection
Bacteria, viruses, and fungi can all cause liver disease. Since bacterial infection is common in many liver problems it is routine to use antibiotics when treating liver problems. Specific diseases include Infectious canine Hepatitis, canine Herpesvirus, Feline Infectious Peritonitis (FIP), Leptospirosis, abscesses, histoplasmosis, coccidiomycosis, and Toxoplasmosis.
Heartworms
These worms can block blood flow into the liver and cause liver failure.
Toxins
There are literally thousands of chemicals that could be toxic to the liver. a few examples of these chemicals that are commonly used to treat ill animals include:
- Rimadyl (arthritis treatment) in Labradors
- Thiacetarsamide (heartworm treatment)
- Ketaconazole (fungal treatment)
- Tylenol (acetaminophen)
- Glucocorticoids (cortisone)
- Anthelmintics (worming medication)
- Parasiticides
- Phenobarbital (epilepsy medication)
Cancer
Cancer can arise directly within the liver (primary) or spread from elsewhere (metastatic or secondary) through the circulatory or lymphatic systems. In the anatomy section we mentioned the dual blood supply to the liver; the portal vein and the hepatic artery. This extra blood supply increases the chance the a tumor in a different organ that has spread into the blood stream will end up in the liver. As mentioned in the physiology section, liver cancer is usually detected only after the disease is well established since functional reserve capacity allowed the liver to function normally for a prolonged period of time.
Metabolic diseases that cause secondary liver problems:
- Hypothyroidism
- Diabetes Mellitus
- Pancreatitis
- Hyperthyroidism
- Cushing’s
Symptoms
Symptoms of liver disease are variable and subtle in the early stages of the problem. The classic symptoms are:
Poor appetite (anorexia)- This is a common symptom
Weight loss- The poor appetite that occurs in liver disease eventually leads to loss of weight. Improper metabolism of fat, carbohydrates, and proteins complicates the situation also.
Polyuria/polydipsia (PU/PD)- This is excess urinating and excess drinking of water. This can occur in liver disease, although several other important diseases cause these symptoms also, notably, kidneydisease, Cushing’s disease, pyometra, and diabetes mellitus (sugar diabetes).
Lethargy- Poor appetite and disruption in normal physiologic processes leads to this symptom. Anemia adds to this lethargy, along with ascites due to the discomfort it causes.
Anemia- Improper nutrition from a poor appetite, along with disease in the hepatocytes will cause this.
Light colored stool- If the biliary tree is prevented from secreting normal bile pigments into the intestine the stool will lack pigmentation and appear lighter in color.
Bleeding disorders- The normal clotting system is impaired since it depends on a healthy liver.
Distended abdomen due to ascites or hepatomegaly. If the distention is severe enough breathing might be labored from pain or the pressure on the diaphragm.
Vomiting (emesis) nausea, or diarrhea. Sometimes blood is present in the vomitus (hematemesis), especially if a gastric ulcer is present. The ulcer comes from a complex interaction of histamine, nitrogen, bile acids, Gastrin, portal hypertension, and altered mucous membrane lining the inside of the stomach. d
Pain due to distention of a diseased liver.
Orange colored urine or mucous membranes due to jaundice.
Behavioral changes- circling, head tilt, heap pressing, and seizures, particularly right after a meal.
Diagnosis
A thorough approach is needed for a correct diagnosis of any liver problem. an organ like the liver that is so intimately involved with other important organs will exhibit symptoms that mimic disease in these other organs. Also, what initially might appear as a diseased liver is in reality a disease elsewhere in the body that is involved with the liver secondarily. This is why it is crucial to follow a thorough and methodical approach called the diagnostic process.
1. Signalment
Liver disease can occur in pets of any age. If it occurs in young animals we tend to think more of toxicity, a liver shunt or a viral disease like adenovirus in dogs, or FIP in cats. In older pets we tend to think more of inflammation and cancer as the cause of the liver problem.
Several canine breeds are prone to getting liver disease:
Bedlington terrier’s, Skye terriers, Doberman pinschers, and West Highland White terriers get a problem with excessive copper accumulation that results from failure of normal biliary excretion of copper.
Cocker spaniels have an increased incidence of chronic hepatitis.
2. History
Early signs of liver disease are subtle, and might exhibit as some of the symptoms described above. It is important to remember that some pets do not show any symptoms early in the course of the disease. This is another reason for yearly exams, along with blood and urine samples in dogs and cats 8 years of age or more.
The recent use of pesticides, insecticides, and drugs might give us a clue. Some Labradors are sensitive to the use of the arthritis medicine Rimadyl. These dogs should have a blood panel analyzed prior to initiating Rimadyl therapy. Every 6 months this panel should be repeated.
A history of poorly controlled diabetes mellitus might also clue us in to liver problems. Pets with liver shunts might have stunted growth and become depressed right after eating. In cats with hepatic lipidosis the history usually involves a lack of appetite (anorexia), especially if the cat was previously obese.
3. Physical Exam
Routine physical exam findings might include:
Distended abdomen due to enlargement of the liver (hepatomegaly). This can be palpated in some situations, especially in the smaller animals. An enlarged liver from a disease other than liver disease can cause hepatomegaly. This includes heart disease and Cushing’s Disease.
Enlarged lymph nodes due to secondary bacterial infections or spread of a primary or metastatic liver tumor.
Bruising (hematoma) might be observed under the skin, or when a blood sample is obtained. This is due to the liver’s affects on the clotting mechanism.
Fever- A rectal temperature of greater than 103 degrees F could accompany liver disease when inflammation or infection is present.
Skin infections and wounds that do not heal, or recur after antibiotics are stopped.
Yellowish discoloration (icterus or jaundice) of the ears, gums, or hairless areas of the skin
Anemia might be observed by checking the mucous membranes for a proper pink color.
4. Diagnostic Tests
Several tests are used as an aid in making this diagnosis.
Blood Panel
A CBC (complete blood count) and BCP (biochemistry panel) should be run on every pet 8 years of age or more, especially if they have any of the symptoms of liver disease.
The CBC might show a decrease in the number of red blood cells (RBC’s). This decrease in RBC’s is called anemia. The white blood cell count (WBC) might be elevated (leukocytosis), normal, or decreased (leukopenia), mostly depending on the cause of the liver problem and how long it has been present.
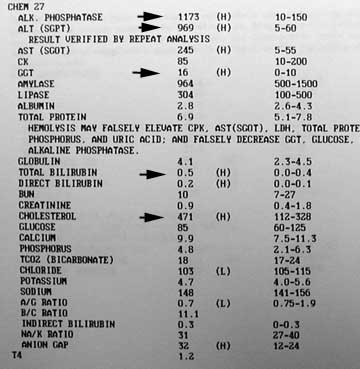
A good way to diagnose liver disease is with the biochemistry panel, abbreviated as BCP. There are several tests on the BCP of dogs and cats that aid us in our diagnosis of liver disease. Many of these are called liver enzyme tests, a few of which we will discuss. When they are elevated it could be a sign of liver disease, but not necessarily so. There are a multitude of conditions that will cause an increase in these enzymes even though the liver is not primarily diseased. (a good example is Feline Hyperthyroidism). They need to be at least 1.5x normal to be of significance. If a pet has significant elevations in the liver enzymes tests then they should be repeated and trends noted. Only then can we get an indication if the liver truly has a problem. To further add to the complication, these tests can be normal in dogs and cats that have severe liver disease.
This older dog has all the classic blood parameters of a dog with liver disease. The alk Phos, ALT, GGT, and Total Bilirubin are significantly elevated. Even the cholesterol is high, which sometimes accompanies liver disease.
Bile Acids
This is liver function test, not an enzyme test, and is not a routine part of the BCP. We will request this test when we suspect a liver problem, whether the enzyme tests are normal or not. This test is performed by taking a blood sample, giving a meal, then taking another blood sample 2 hours after the meal. Comparing the pre-meal and post-meal blood results gives us valuable information. The bile acids test is an accurate measure of liver function.
![]()
Urinalysis
A urine sample can give us important clues as to the existence of liver disease. The specific gravity might be below normal, an indication that PU/PD is present. Bilirubin might be present, a finding that is always abnormal in cats. There also might be ammonium biurate crystals, a sign of improper ammonia metabolism found in Hepatic Encephalopathy.
Abdominocentesis
Analysis of the fluid obtained from a pet with ascites can give valuable clues as to its cause. There are numerous causes to ascites, some of the more common ones are heart disease, liver disease, and cancer.
Fluid is removed from the abdomen with a special needle and syringe.

Liver Biopsy
This is a very valuable test in the diagnosis of liver disease. a sample of the liver can be obtained during an exploratory surgery or during an ultrasound procedure. The pathologist can look at the hepatocytes microscopically and determine if disease is present and what the cause is.
It is helpful to run a coagulation panel prior to any liver biopsy. A diseased liver might not be able to clot properly, and a biopsy could cause hemorrhage into the abdomen.
Stool
A dog that excretes stool without normal pigmentation could indicate liver disease. It occurs when there is obstruction of the biliary system and normal bile pigments are not secreted to cause the normal dark color of stool.
Radiography
An enlarged liver on a radiograph is called hepatomegaly, an abnormally small one is called microhepatica. Either one can be a sign of a liver problem.
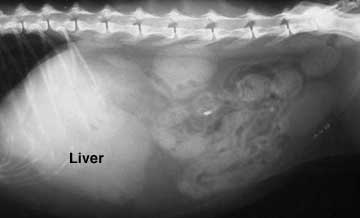
The liver in this radiograph is enlarged because the edge of the liver is protruding far beyond the last rib. The edges of this liver are very sharp and clearly outline its borders.

Some radiographs of a liver with hepatomegaly don’t show the routine shape of the liver lobes. This case of a liver cancer has a very rounded appearance. an tumor of the stomach, spleen, or intestines can also have this appearance.
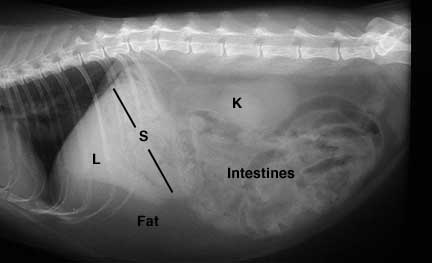
Sometimes we diagnose hepatomegaly or microhepatica indirectly by looking at the angle of the stomach This picture shows the angle of the stomach in a normal radiograph of the abdomen.
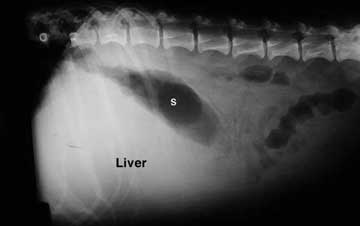
This liver is pushing the stomach (S) towards the rear, an indication of hepatomegaly, even though it is difficult to clearly see the liver.
Ultrasound
Ultrasound is highly beneficial in the diagnosis of liver disease. We recommend ultrasounding a liver when the liver enzymes tests are elevated over time, or the bile acids test is abnormal.
The internal structure (called parenchyma) can be analyzed, and post hepatic liver disease can be differentiated from hepatic liver disease. This can be very important because disease in the liver can often be diagnosed with a biopsy during the ultrasound. Post hepatic liver disease is diagnosed and treated with an exploratory surgery (called a laparotomy).
This liver ultrasound reveals a mass in the liver. Can you see its circular appearance at the arrow? It also shows abdominal effusion (this is the ascites described previously).

Exploratory Surgery
Being able to literally look at the liver and palpate individual liver lobes is sometimes needed to confirm a diagnosis of a problem. Taking a biopsy of a diseased part of the liver is enhanced this way.
This picture is from an exploratory surgery (called a laparotomy) on a cat with kidney cancer. We are looking at the liver for any sign of problems- this one is healthy. It is obvious that a laparotomy gives us a great view of the liver.

5. Response to Therapy
The liver has tremendous ability to recover from a disease and literally regenerate hepatocytes. If we treat a liver problem that we diagnosed as treatable, and the liver does indeed recover, then we probably made the correct diagnosis.
In many general problems our doctors recommend Hills Prescription diet K/D or I/D.
Liver Diseases
There are a large number of diseases that affect the liver. We will discuss a few of the most common ones.
Hepatic Lipidosis Pathogenesis
A small amount of fat is normally present in hepatocytes. The original source of this fat is from the diet. From the intestines (remember, bile needs to be present for this to occur) it is absorbed into bloodstream, binds to albumin and is presented to hepatocytes. This fat is in several forms, the main ones being cholesterol, triglycerides, and fatty acids.
Fat is used for energy, the production of sex and steroid hormones, and in cell wall integrity, and as storage for future energy needs. In a normal liver the rate at which the fat from the bloodstream enters the liver and the rate at which the liver utilizes this fat is roughly equal. When there is an imbalance between the rate of deposition of fat in hepatocytes and the rate of utilization of this fat, the amount of triglycerides builds up and lipidosis results. In many species this excess of fat in the hepatocytes causes no serious problem, not so in cats.
The exact mechanism that causes this imbalance in cats is unknown. It is speculated that excess fat stores in obese cats overwhelm the liver when these fat stores are needed for energy (a cat that is not eating or is starving). This sets off a cascading series of events that involve insulin, glucose, and the enzyme lipase, leading to excess accumulation of triglycerides in hepatocytes.
Primary
This disease, seen more often in cats than in other animals, occurs when excess fat (called triglycerides) accumulates in liver cells (hepatocytes) and bile accumulates in hepatocytes (cholestasis). It is technically called Idiopathic Hepatic Lipidosis (IHL). The idiopathic part means that the specific cause is unknown. This form of lipidosis causes liver failure, and can lead to death if left untreated.
Secondary
In this form of hepatic lipidosis the fat accumulation occurs secondary to some other problem. This is more common than primary hepatic lipidosis. Some of the more common causes are:
- Diabetes Mellitus
- Tetracycline antibiotics
- Inflammatory Bowel Disease (IBD)
- Pancreatitis
- Malnutrition or even starvation
- Obesity
- Hyperthyroidism
- Kidney disease
- chronic cystitis
- Cancer
- Cardiomyopathy
Secondary hepatic lipidosis does not cause liver failure. When the primary disease is treated the liver problem tends to resolve. A large percentage of cats have hepatic lipidosis secondary to these diseases (and others).
Signalment
IHL can occur in any age or breed of cat, although it is not commonly seen in young cats. It is the most common liver disease found in cats.
Toy breed dogs can get a lipidotic liver after fasting or not eating for a period of time. They become hypoglycemic (low blood sugar), and can even die.
History
Cats with IHL consistently have anorexia (not eating), leading to weight loss. They are usually (or were) obese, and sometimes there is a history of a recent stressful episode that caused them to stop eating. Many owners will notice jaundice (icterus) and vomiting. Other symptoms could include diarrhea, constipation, salivation, and depression.
Physical Exam
Cats with IHL have lost weight (although they could still be obese when examined) and may have yellowish discoloration (icterus) on the ears, the whites of the eyes, and the oral mucous membranes (gums). An enlarged liver (hepatomegaly) might even be palpated. Some of the other common signs of liver disease as described previously might be present on occasion.
This cat has icterus (jaundice) of its oral cavity from hepatic lipidosis, although a severe enough anemia could also cause this appearance.

This is the way the blood looks just after it was obtained on this cat and spun down in our centrifuge. The serum, which is the top layer, has the same yellowish-orange appearance as this cats gums.

Diagnostic Tests
A blood panel will commonly show highly elevated levels of ALT and Alk Phos, and mild elevations in GGT. In addition there are commonly high levels of bilirubin in the bloodstream and the presence of bilirubin in the urine. A bile acids test is frequently elevated, and the blood ammonia level might also be elevated on occasion.
Other findings could include anemia, low albumin (hypoalbuminemia), high cholesterol (hypercholesterolemia), low BUN, low potassium (hypokalemia), and high glucose (hyperglycemia).
Diseases that can mimic IHL in cats include FIP, cholangiohepatitis, and liver cancer. A biopsy of the liver (usually performed when the ultrasound is done) is needle to verify the diagnosis. IHL usually involves many hepatocytes, so a general sample of the liver tissue usually yields diagnostic results. This is not the case with all liver diseases though. Some are focal and involve only a small portion of the liver. Fortunately, the ultrasound can pick up these focal areas and a biopsy needle can be directed to the diseased area by the ultrasound.
Radiography
Radiography might show hepatomegaly or a normal sized liver. Weight loss might be apparent on the radiograph, yet abdominal fat stores might be normal.
Ultrasound
Ultrasound reveals hepatomegaly with telltale changes of the liver parenchyma (internal anatomy of the liver). Ultrasound might also show inflammation of the pancreas (pancreatitis).
Exploratory Surgery
If an exploratory surgery is performed the liver might appear tan or yellowish in color, enlarged, and with swollen borders. It is greasy to the touch and easily injured. Exploratory surgery allows us to take a large section of the liver for biopsy. It also allows visualization of other abdominal organs, particularly ones that might be implicated in this disease like the pancreas.
Histopathology
This is the only way to confirm the diagnosis.
Treatment
Supportive care is crucial, and may have to be instituted for a prolonged period of time. Cats with IHL should be kept in the hospital until they are taking all medications well and their blood parameters are improving.
Fluids and Electrolytes
This corrects the dehydration that occurs with a poor appetite and supplies needed sodium, potassium, and chloride. This fluid is usually given intravenously (IV) at first. It can be given subcutaneously (SQ) at home after the initial dehydration is corrected. B-Complex vitamins are routinely added to the fluid bag to correct of a deficiency that can occur with IHL. Vitamin K might be needed in cats with clotting problems. This deficiency might be due to anorexia and reduced synthesis by the atrophied intestines. Simultaneous with fluid therapy we will begin caloric support.
Caloric Support
This is the most important part of treatment for IHL, and usually involves the use of a feeding tube. It is so important that we have devoted a full page to it.
Cats need at least 60 Kcal/kg/day of caloric dense high protein diet. The lining of the small intestines (called villi) will atrophy due to a lack of use, so a short adaptive period is needed to get them functioning properly again. This is done by feeding small amounts of food for the first few days, even though full caloric requirements are not being met.
The protein level of the diet should not be restricted unless they are showing obvious signs of hepatic encephalopathy (HE).
Appetite stimulating drugs (valium, periactin) have no place in hepatic lipidosis due to their ineffectiveness, and some of them might even predispose cats to hepatic encephalopathy (HE).
Human enteral diets do not have adequate protein, arginine, or taurine for cats.
Antibiotics
A weakened immune system predisposes these cats to infections, along with the stress of diagnostic tests, hospitalization, and treatment. Antibiotics will help in this situation, especially if mental depression is present from hepatic encephalopathy (excess ammonia in the bloodstream). Antibiotics minimize the bacteria count in the colon, thus reducing the amount of ammonia that is absorbed from the intestines into the bloodstream.
Tetracycline antibiotics should be avoided if possible because they could be an initiating cause of hepatic lipidosis.
Lactulose
This drugs helps minimize the ammonia buildup that leads to vomiting, salivation, and mental depression.
Anti-vomiting medication
Drugs like Reglan can control vomiting and minimize gastric bleeding due to ulcers. As a general rule we want to minimize the use of valium and cortisone in cats with IHL.
Ulcer Medication
Medications like Tagamet and sucralfate will help protect the stomach lining and make pets feel much better. These pets are more inclined to eat.
Supplemental Treatment
Some cats might benefit from other treatment modalities, although this is not the case in all cats. The mechanisms of action of these supplements are postulated but not proven.
L-Carnitine- This essential amino acid is required for proper fat utilization by the liver. Even though low levels are not found in cats with IHL, supplementation might be beneficial.
Arginine- This is another amino acid. It comes from muscle protein when cats are fasted. after a prolonged fast the muscle is depleted of protein and a deficiency of arginine might occur. A deficiency might lead to high levels of ammonia and eventually hepatic encephalopathy (HE). It is an essential amino acid in the cat.
Taurine- This is also an amino acid that could be involved with IHL. It is an essential amino acid, so supplementation might be helpful.
Ursodiol- This drug has an affect on how the liver metabolizes cholesterol and decreases the toxic effects of bile.
When the appetite starts to return we will slowly decrease the volume of food given via tube feeding. When your cat is eating well on its own, and the liver tests have improved on the blood panel, we will remove the feeding tube. This can be anywhere from several days to several months.
Prognosis
This disease is reversible in most cases when treated medically. Cure rates range from 65% to 75% when treatment is started early enough.
Cats that have pancreatitis, remain persistently hypokalemic (low potassium), or whose elevated bilirubin does not decrease significantly within 10 days have a guarded to poor prognosis.
Monitoring
Changes can occur rapidly during the early phases of treatment, so blood parameters need to be routinely monitored, especially electrolytes like potassium and phosphorous. Phosphorous, potassium, and red blood cell levels should be monitored for the first 72 hours after initiating caloric support. Serum enzymes and bilirubin should be monitored weekly until appetite returns.
Prevention
Even though the specific cause of IHL is unknown, obesity is a known predisposition. Since obesity is controllable you can dramatically reduce the chance of your cat getting IHL by keeping it at a proper weight.
Early treatment dramatically increases the chance of recovery, so if your cat does not eat for 24 hours it should be brought to our clinic for an exam and blood testing.
Portosystemic Shunt (PSS)
Pathophysiology
Ammonia comes from bacteria in the intestines and when muscles utilize protein as a energy source. In a normal animal this ammonia gets delivered through the portal vein directly into the liver. The liver cells metabolize the ammonia to urea, which is excreted by the kidneys. The liver also detoxifies bacteria and drugs that are also absorbed from the intestines before they get into the general circulation and go to the rest of the body.
Shunts occur when the blood supply through the liver is abnormal. The abnormal blood vessel shunts blood around the liver instead of through the liver. By bypassing the liver the toxins that are normally metabolized by the liver (especially ammonia) are allowed to enter the general circulation before the liver has a chance to detoxify them. It is this ammonia buildup that causes most of the symptoms observed with PSS. It is also know as hepatic encephalopathy (HE) because of its toxic effects on the brain.
Several factors can add to HE. A diet high in protein will add to blood ammonia levels, along with infection, cancer, and excess use of cortisone. Kidney disease along with constipation will also add to the problem. Some drugs, notably barbiturates, valium, and anesthetics can also be factors.
Shunts can be multiple or single. The shunt can occur within the liver (intrahepatic) or in the blood supply before it enters the liver (extrahepatic). Larger breed dogs are more prone to intrahepatic shunts, extrahepatic shunts are more common in small breed dogs and cats. It is important to differentiate them for therapeutic purposes.
There are other diseases that can mimic PSS. They include liver toxins, liver infection, liver cancer, and hepatic lipidosis (see previous description). An organ as complex as the liver necessitates the need for a precise diagnosis before treatment can be instituted. Also, a pet with chronic liver disease leading to cirrhosis will sometimes get acquired shunts.
Causes
Congenital The congenital version of PSS occurs more commonly in dogs than in cats. Most of these shunts are extrahepatic, meaning the shunting vessels are located outside of the liver.
Acquired.
Seen mostly in dogs, they occur when there is increased resistance to blood flow through a fibrotic liver. These shunts occur inside the liver and are not easily corrected.
Signalment
Congenital shunts tend to be found in younger dogs and cats, while acquired shunts tend to occur in older animals. In some situations the symptoms of this disease are so subtle that a diagnosis of congenital shunt is not made until a pet is much older. We tend to see it more often in male cats as opposed to female cats.
Several dog breeds are predisposed:
- Irish wolfhounds
- Maltese
- Yorkshire terriers
- Miniature schnauzers
- Australian cattle dogs
- Retrievers
- Cairn terriers
- Old English sheepdogs
Cat breeds might include:
- Himalayan
- Persian
History
Some of the symptoms of PSS can be subtle, and easily interpreted as a quiet puppy or kitten. Symptoms can wax and wane, thus they are easily missed and can be subtle. Some pets seem to have a preference for fruits and vegetables.
Behavior changes, particularly right after eating. These changes include depression, head pressing, blindness, lethargy, coma, seizures, and personality changes. anorexia, vomiting, diarrhea, and excess salivation (more so in cats) might be present. Excess urinating and drinking (PU/PD), blood in the urine (hematuria) and an increased incidence of ammonium urate bladder stones might also be present. Other symptoms might include inhibited growth, fever, and abnormally long recovery periods from anesthesia (ex.-when a spay or neuter is performed).
Physical Exam
Pets with PSS will commonly be stunted in growth, but usually no abnormalities on their neurologic exams. A small liver might be palpated on smaller animals. Hair coat might be unkept and there might be ascites on abdominal palpation. Other occasional findings include cryptorchidism.
Diagnostic Tests
Several diseases mimic PSS. They include Distemper, FIP, toxoplasmosis, FeLV related diseases, toxicities, idiopathic epilepsy, and hypoglycemia. This emphasizes the importance of proper testing to come to an accurate diagnosis.
Blood Panel
In dogs, a blood panel might show anemia along with elevated levels of ALT and Alk Phos. The BUN might be low, the protein level might be low (hypoproteinemia), the blood sugar might be low (hypoglycemia) in the smaller breed dogs, and the cholesterol might also be low. A bile acids tests will show an elevation, particularly after we feed a meal. If we suspect PSS as the cause to your pets problem we will run a blood ammonia level, which will come back elevated if PSS is present. An ammonia tolerance test might be needed for verification.
In cats the albumin, BUN, and cholesterol might be low or at the low end of the normal range.
Urinalysis
A urinalysis might show symptoms of urinary tract infection or abnormal crystals, particularly ammonium biurate.
Radiography
A radiograph of the liver might show a small liver (microhepatica), particularly in the dog. The liver might be hard to evaluate because a lack of abdominal fat, due to emaciation or a young animal.
Kidney changes and bladder stones might be visible, although ascites might obscure vision of internal organs. ammonium urate bladder stones might not show up on a radiograph even though they are present.
Ultrasound
Ultrasound can give further information on the liver and its blood supply, and even detect ammonium biurate bladder stones which normally don’t appear on a radiograph. Ultrasound is better at differentiated intrahepatic shunts as opposed to extrahepatic shunts.
Positive Contrast Portography
Some consider this test the gold standard for diagnosis. In this test a special dye is injected directly into one of the veins of the small intestines while a pet is under anesthesia. A radiograph is taken and the flow of the dye is followed. If a shunt is present this will show up on the radiograph.
Biopsy
A biopsy of the liver (usually performed when the ultrasound is done) will show microscopic abnormalities consistent with PSS. This usually includes small hepatocytes and a decrease in the blood vessels within the liver.
Laparotomy
Exploratory surgery to visualize the vessels directly, or to inject dye into the portal vessels, is also used to verify the diagnosis. After the dye is injected a radiograph is taken to assess absorption. Surgical repair can immediately be initiated.
Scintigraphy
A transcolonic nuclear scan can give a definitive diagnosis. In this test a small amount of radioactive (99technetium pertechnetate) material is put into the colon and its absorption is monitored. In pets with PSS this radioactive material will appear in the heart before it appears in the liver, the opposite of what should normally happen. This test does not require anesthesia like the Positive Contrast Portography test.
Treatment
Medical
Fluids and Electrolytes
This corrects the dehydration that occurs with a poor appetite and supplies needed sodium, potassium, and chloride. This fluid is usually given intravenously (IV) at first. Pets that are severely ill from PSS should not be given anything orally initially.
Cleansing Enemas
Enema’s will decrease the bacterial count of the intestines, leading to less ammonia absorption.
Lactulose
Lactulose works in the large intestine to minimize the production of ammonia by bacteria. It does this by changing the pH and converting ammonia to a form that is not readily absorbed into the bloodstream. It also stimulates normal colon bacteria to absorb ammonia, which is then passed in the feces. Finally, it stimulates the intestines so that ammonia passes through faster, which means there is less time for absorption.
Antibiotics
These drugs are also administered, especially if mental depression is present. They minimize the bacteria count in the colon, thus reducing the amount of ammonia that is absorbed from the intestines into the bloodstream. They work well with lactulose to decrease the ammonia level.
Dietary Modification
A diet that is restricted in protein may be beneficial because less ammonia is produced as a by-product of metabolism. This protein needs to be of high biological value, such as eggs and dairy products. Meat based proteins should be avoided since they can increase the chance of HE. Most of the caloric needs of a pet with PSS should be supplied with carbohydrates like rice and pasta. Higher fiber diets might also be helpful, as long as the dog or cat is not undernourished. They can act to minimize ammonia production and absorption in a manner that is similar to lactulose.
Surgical
For most PSS cases surgery is the treatment of choice. The abnormal vessel that is shunting blood around the liver is identified and closed (ligated) to minimize blood flowing through it. When the abnormal blood vessel is ligated blood will now flow through the liver instead of around it. This is readily accomplished for solitary extrahepatic shunts. Intrahepatic shunts can be more difficult to identify and ligate. Post surgical monitoring is important. If the pressure within the liver becomes too high due to the increased blood flow through the liver then the ligation on the shunting vessel(s) must be reduced or removed.
In some cases medical management must also be utilized to affect a cure. The final outcome of treatment depends on what age the PSS started, how long it has been present, and whether it is intrahepatic (worse prognosis) or extrahepatic in nature.
Long Term Monitoring
Pets on long term medical care need to be monitored carefully. Body weight, albumin, and total protein are watched to ensure adequate protein in the diet. Initially these tests should be performed monthly, then every 3 months. In addition to the above tests, bile acids are monitored monthly, then every three months to assess the vitality of the liver. Blood ammonia levels are monitored monthly to assess effectiveness of treatment. When stable, ammonia levels can be monitored every 3 months.
Prognosis
Many pets with isolated extrahepatic shunts return to a normal life after surgery. There is no guarantee that surgery will correct the problem, especially those pets that develop the disease very early in life. Some of them will need medical management simultaneously. The prognosis for pets that are treated only medically varies. Cats do not do as well as dogs when surgery is attempted.
Chronic Active Hepatitis
This disease is also known as Chronic Canine Inflammatory Hepatic Disease (CCHID). It is a series of different liver diseases with similar characteristics when analyzed under the microscope (histopathology). It has similarities to cirrhosis found in humanoids.
Cause
Usually unknown. In some cases an infection caused by a bacteria called Leptospirosis or a virus called adenovirus is the cause. We protect dogs from this adenovirus when we give a DHLPP vaccine. The “H” stands for hepatitis caused by the adenovirus. This same vaccine can also protect dogs from Leptospirosis.
Pathophysiology
The immune system makes antibodies that affect liver cells. Toxic compounds add to the problem. Some of these compounds include cholesterol, iron, copper, and toxins located within the blood vessels. All of this leads to inflammation, and the eventual replacement of normal liver cells (hepatocytes) with fibrous tissue. Eventually, the blood flow through the liver is compromised, the blood pressure at the liver is elevated (hypertension), and numerous extrahepatic PSS’s develop (see PSS above). The body then shows signs of fluid buildup in the abdomen (ascites) and HE (see above). After a variable period of time liver failure often results.
Signalment
It tends to occur more often in older animals.
Several dog breeds are predisposed:
- Doberman Pinschers
Most common in middle-aged females with improper copper metabolism.
- Cocker spaniels
Most often in older males. Typical symptoms include fluid buildup in the abdomen (ascites) and low albumin (hypoalbuminemia) on a blood sample.
- West Highland white terriers, Bedlington terriers, and Skye terriers.
It is associated with copper accumulation in hepatocytes, sometimes seen more often in young dogs.
History
Symptoms are vague, and come and go until the disease progresses. The typical symptoms of liver disease are present, and include PU/PD, anorexia, vomiting, diarrhea, ascites, icterus, and HE. Ulcers of the stomach can occur and lead to vomiting blood (hematemesis)
Other symptoms can involve the blood system, and include bleeding disorders and vomiting blood (hematemesis). This is because the liver is involved with the production of clotting factors (remember the physiology section above?). In occasional cases the opposite occurs, and the liver causes excessive clotting of blood. This predisposes animals to a problem known as disseminated intravascular coagulation (abbreviated as DIC).
Physical Exam
An exam of a pet with this disease can vary from normal to many abnormalities. Some of the abnormal findings are described in the liver exam findings above.
Diagnostic Tests
Blood Panel
A blood panel will commonly show anemia along with elevated levels of ALT and Alk Phos. There might also be an elevation in cholesterol, a decrease in BUN, glucose, and albumin. There might also be an increase in bilirubin, ammonia, and bile acids.
Urinalysis
A urinalysis might show symptoms of urinary tract infection or abnormal crystals, particularly ammonium biurate.
Radiography
A radiograph of the liver might show an enlarged liver (hepatomegaly) initially, eventually in might progress to a small liver (microhepatica).
Ultrasound
Ultrasound is the best way to make this diagnosis. The internal architecture (parenchyma) can be analyzed and a biopsy can be obtained with relative ease. In some cases it is important to know the coagulation status of the blood with a special blood panel prior to obtaining this biopsy. In many cases ultrasound is preferable to exploratory surgery since some of these animals are not good anesthetic risks and the procedure is much less invasive.
Laparotomy
The liver can be thoroughly visualized and palpated during an exploratory surgery. A biopsy can easily be obtained, and post biopsy bleeding can be monitored.
Biopsy
Samples of the liver taken with either a biopsy needle during ultrasound or during a laparotomy will be analyzed microscopically by a pathologist to make a definitive diagnosis and to look for a cause if possible.
Treatment
Fluids and Electrolytes
This corrects the dehydration that occurs with a poor appetite and supplies needed sodium, potassium, and chloride. This fluid is usually given intravenously (IV) at first. It can be given subcutaneously (SQ) at home after the initial dehydration is corrected. B-Complex vitamins are routinely added to the fluid bag. Care must be taken not to give excessive amounts of fluids, especially if they contain sodium, in pets with fluid buildup in the abdomen (ascites).
Treating the Cause (when known)
Antibiotics are used to control bacterial infections and drugs that are suspected of causing this disease are stopped. We tend to use antibiotics that have minimal need for liver metabolism in order to minimize their toxic effects.
Rest
The liver has ability to heal itself if the disease is not too well entrenched. Rest can be a big aid, along with proper nutrition. A diseased liver needs calories, which sometimes need to be supplied with afeeding tube.
Ascites Reduction
Sodium restriction helps minimize fluid buildup (ascites) in the abdomen. This can be accomplished using Hills K/D Prescription Diet. Diuretics like Lasix are also used to help pull this fluid out of the abdomen.
Dietary Modification
Use a diet that is restricted in protein may be beneficial because less ammonia is produced as a by-product of metabolism. This protein needs to be of high biological value, such as eggs and dairy products. Hills Prescription Diet K/D is the diet of choice. Meat based proteins should be avoided since they can increase the chance of HE. Higher fiber diets might also be helpful, as long as the dog or cat is not undernourished. This is the same basic diets as for pets with PSS (see above).
Ulcer Treatment
This will make pets more comfortable, more inclined to eat, and prevent bleeding in the stomach.
Liver Specific Drugs
Corticosteroids- Cortisone is used if there is evidence that the immune system is implicated as a cause of the liver problem.
Ursodiol- This drug replaces toxic bile acids with a type of bile that is less toxic.
Zinc- Supplementation might help reduce the effects of copper toxicity.
Long Term Monitoring
CCHID monitoring is similar to PSS (see above). In addition, repeating a liver biopsy 6 months after initiating therapy used.
Infectious Canine Hepatitis (ICH)
Background
The disease is called hepatitis because liver cells are one of the prime targets. It is caused by an adenovirus that is found world wide and affects mainly in the dog family (canids). The virus is very resistant to disinfectants and can remain infectious in the environment. Many dogs get exposed to this virus, develop antibodies, and show no symptoms of the disease. Spread of this virus is usually orally and nasally, but can also be spread by utensils and external parasites. Within 7 days of exposure most dogs develop an adequate antibody response to protect the liver and other organs.
Symptoms
ICH can occur in unvaccinated dogs of any age, but usually occurs in dogs under one year. In the more severe cases vomiting and diarrhea can occur. These dogs can also have fever, coughing, swelling of the head and neck due to lymph node enlargement, abdominal tenderness and even central nervous system signs. These symptoms may last up to one week, and can be prolonged by other concurrent diseases like Distemper. A syndrome of this disease can cause rapid death leading people to conclude that the dog was poisoned. Dogs that show minimal symptoms can show ocular lesions during the convalescent phase. In uncomplicated cases these eye lesions heal completely.
Diagnosis
Blood samples give a clue to this disease but are not diagnostic. White blood cells can be low, liver enzyme tests may be elevated, and clotting factors can be disrupted. These findings with previously described history and physical exam findings are how the disease is usually diagnosed. Antibody tests are available but are not routinely used to make a diagnosis.
Treatment
Like most viral diseases therapy is directed towards symptoms. When symptoms are severe enough, intravenous fluids are administered. Since clotting factors can be disrupted, particular attention needs to be paid to bleeding problems. If bleeding problems are severe enough, a whole blood transfusion must be administered. Dogs that are comatose may need intravenous glucose.
Prevention
Most pups receive adequate antibodies from the bitch, which can last up to 4 months. Vaccines are highly effective and can confer long term protection. Two vaccines need to be given at 3-4 weeks apart beginning at 8 weeks of age. The DHLPP (Distemper-Hepatitis-Leptospirosis-Parainfluenza-Parov) vaccine contains protection against this adenovirus. The DHLPP vaccine is also known as the Da2PL. The a2 part stands for adenovirus.
A picture of our vaccine label

Copper Toxicosis (Copper Storage Disease)
The level of copper in the body is maintained by the excretion of bile. In this disease copper accumulates in hepatocytes, eventually causing inflammation and scarring, ultimately leading to liver failure (similar to CCIHD above). Excess copper released from the liver can cause hemolytic anemia.
Signalment
It is common in certain breeds:
Bedlington terriers- They have a genetic defect in how they metabolize copper and how it is excreted in the bile. This leads to excess accumulation in hepatocytes.
West Highland white terriers- They have a similar genetic defect as Bedlington terriers, but the copper accumulation is not as severe and does not always lead to liver failure.
Some Dobermans and Skye terriers with chronic liver disease also have elevated levels of copper in their hepatocytes. The copper accumulation in the liver might be a cause of the chronic hepatitis that eventually results, or an effect of a pre-existing hepatitis.
History
Bedlington’s with copper toxicity have minimal symptoms early in the disease. In the acute form, seen in younger dogs, symptoms include lethargy, anorexia, and vomiting. Death can occur in 2-3 days. Middle aged or older dogs have a more chronic course. Eventually symptoms of liver failure appear, including anemia, depression, lethargy, and anorexia.
Physical exam
Anemia might cause pale mucous membranes. There might also be icterus due to both anemia and liver failure. These dogs will also be weak and underweight.
Diagnostic Tests
A blood panel will commonly show elevated levels of ALT, GGT and Alk Phos, in addition to high levels of bilirubin in the bloodstream and the presence of bilirubin in the urine. A bile acids test is elevated and radiography reveals a small liver. This disease is diagnosed by liver biopsy.
Treatment
Treatment has two goals: Enhance excretion of excess copper, and minimize further absorption of copper from the intestines.
Chelating agents Drugs like penicillamine bind with copper to allow easier excretion.
Zinc
Zinc will help minimize further copper absorption from the intestines.
Supportive Care
Similar to other liver diseases previously described
Long Term Monitoring
Serum enzymes and bilirubin should be monitored at least every 6 months
Prevention
Bedlington terriers should be screened at 1 year of age. Treatment at this early age leads to a good prognosis.
Cancer (Neoplasia)
A benign tumor is called and adenoma, a malignant one is a carcinoma.
Primary- Arising directly from the liver
- Adenoma
- Carcinoma
- Hemangiosarcoma
- Hemangioma
- Leimyosarcoma
- Fibrosarcoma
- Fibroma
- Osteosarcoma
They can arise directly from the hepatocytes where they are called hepatocellular. If they arise from the biliary system they are called cholangiocellular. Dogs get more hepatocellular, cats get more cholangiocellular. The cause of these primary neoplasia’s is unknown in most cases.
Secondary- From another organ that has spread to the liver
- Lymphosarcoma
- Mast cell
- Pancreatic carcinoma
- Myeloproliferative
The organs that commonly are the source of these cancers include:
- Pancreas
- Lymph nodes
- Spleen
- Mammae
- Adrenal glands
- Bone and bone marrow
- Lungs
- Thyroid
- Intestines
Secondary, also know as metastatic, liver cancers are much more common than primary.
Signalment
Cancer is found in most animals and most breeds. It tends to be found mostly in older animals.
History
Almost any sign of illness can potentially be attributed to neoplasia. Common ones include anorexia, lethargy, weight loss, PU/PD and vomiting.
Physical Exam
Exam results of animals with liver neoplasia mimic the results found in other liver diseases.
Diagnostic Tests
A blood panel will commonly show elevated levels of liver enzymes, in addition to high levels of bilirubin in the bloodstream and the presence of bilirubin in the urine. A bile acids test is elevated and ultrasound reveals hepatomegaly (enlarged liver) with telltale changes of the liver parenchyma (internal anatomy of the liver). Ultrasound might also show inflammation of the pancreas (pancreatitis). A liver biopsy is needed for a definitive diagnosis. There is an ultrasound picture of liver cancer in the diagnostic section above.
Treatment
Primary hepatic neoplasms are treated by removal of the affected liver lobe when possible. If multiple lobes are involved then surgery is usually not performed. Secondary hepatic neoplasms are treated with chemotherapy. The results vary, and depend on the duration, location, and degree of malignancy of the neoplasia. The prognosis is poor for long term survival.
Supportive care that is similar to other liver diseases is also used in neoplasia
Prevention
Since the cause is usually unknown prevention is difficult. Good nutrition and lots of TLC are always important in preventing any disease.