
The cardiovascular system is complicated, very complicated, so pace yourself on this page. It starts easy enough, but it does not stay that way, even though you will be given only a brief summary of the anatomy and physiology of the cardiovascular system.
This page is broken down into four sections:
- Cardiac Muscle
- Thoracic Anatomy
- Cardiac Physiology
- Cardiac Pathophysiology
Cardiac Muscle
The body contains three different types of muscle:
Skeletal Muscle
The muscle type we usually think about when we mention muscles. Skeletal muscles provide locomotion and movement- the biceps muscle to move our arms, or the quadriceps muscles to move our legs. These muscles perform their action due to conscious control of our brains. Your arm does not automatically shoot a free throw until you tell it to do so (even when Dr. P tells his arm to shoot the free throw it doesn’t always work as planned).
Smooth Muscle
Smooth muscles tend to perform their functions automatically without any conscious thought on our part. You don’t tell them what to do, they do it on their own, under the control of the autonomic nervous system (ANS). The muscles that surround arteries to make them constrict or dilate are smooth muscles. The muscles of the intestines that push the food along (a process called peristalsis) are made of smooth muscle.
Cardiac Muscle
It only resides in the heart. Cardiac muscles have their own supply of electricity, and “fire off” on their own without any stimulation.

This is a close-up view of the heart muscle (myocardium) in the left ventricle of a dog. It is thick because this dog’s heart has to spend a lifetime pumping blood to all the cells of the body. Later on when we talk about cardiomyopathy it is this muscle that is affected.
How does the heart beat all by itself? It accomplishes this feat because each heart cell supplies its own electricity. To make a complicated story a little simpler, it has to do with how the heart cells retain or excrete potassium, sodium, and calcium ions.
When sodium and calcium are pumped out of the heart cell, potassium is pumped in. This eventually creates an imbalance in their equilibrium, with many more sodium and potassium ions outside of the heart cell than inside. This creates a “positive” charge outside of the heart cell, and the heart cell is now “polarized” (remember this word when we discuss electrocardiograms).
The body eventually wants to correct this imbalance of sodium, calcium, and potassium. So the opposite occurs. Potassium rushes out while the sodium and calcium rush in. The cell is now depolarized, and will stay that way until the positive charge outside the cell again reaches a threshold and the flow once again reverses.
Every time this reversal of flow occurs, it generates a spark of electricity which races through the heart. It is this electrical spark that causes heart cells to contract and the heart to beat.
Electrical System
Even though they beat on their own, the electrical activity in each heart cell needs to be coordinated if the 4 heart chambers (2 atria and 2 ventricles) are to pump an adequate amount of blood in the proper direction. Later on, when we talk about electrocardiograms, it is this electrical conduction we will be referring to.
At the beginning of the right atrium there is an anatomical structure called the sino-atrial node (SA Node). It is the leftmost red circle on the diagram below. It is this area of the heart muscle that originates the coordinated beating of the heart. When this SA Node fires off it sends electrical impulses (the wires that carries these impulses are called perkinje fibers) through both atria, causing them to contract at the correct time.
One of the signals from the SA Node also stimulates the atrio-ventricular node (AV Node), the second red circle below and to the right of the SA Node below. Stimulation of this node stimulates nerve fibers that surround the ventricles, causing them to contract in a rhythmic way. There are other factors involved, especially hormones and other parts of the nervous system.

It all starts with the SA node at the right atrium
The atrio-ventricular bundle (AV bundle) is also known as the bundle of His in honor of the man who discovered it. Since the heart in a dog or cat beats approximately 2 times every second, these nodes have to fire off rapidly if everything is to stay coordinated. From the time the SA Node fires it takes only 0.22 seconds for the ventricles to contract.
The SA node is called the pacemaker because it depolarizes at a faster rate than any other group of cells in the heart, and imposes that faster rate on the heart as a whole. If for any reason the SA node stops beating, the AV node, which has the next fastest rate of depolarization, would become the heart’s pacemaker. Your heart might beat at a slower rate, but at least it would keep on beating in the coordinated fashion between atria and ventricles that is necessary for adequate blood flow.
If the AV node failed, the AV bundle would take over. If it failed, the Perkinje fibers would start the heartbeat, and if they failed as well, a group of cells somewhere else in the heart would start pulsing. However, the further away the heart gets from its normal pattern and rate of beating, the less blood it pumps and receives, until eventually it can no longer sustain life. This is called a heart block, and is diagnosed by an electrocardiogram (EKG or ECG).
Abnormalities in the heart’s normal rhythm, known as arrhythmias, are a common problem in heart disease. Arrhythmias can be minor and unimportant, or severe and life threatening. There are many different kinds of arrhythmias, including:
Tachycardia – An abnormally fast heartbeat. If the heart beats too fast is does not spend enough time in diastole. The heart chambers do not have enough time to fill up enough with blood, so the heart does not pump out an adequate amount of blood for the needs of the cells at the next systole (contraction). In addition, the lack of time in diastole causes the heart muscle itself (myocardium) to suffer since it is in diastole that blood flows from the coronary arteries into the heart muscle.
Bradycardia – An abnormally slow heart beat. If the heart beats too slowly the blood pressure decreases and it does not generate enough flow of blood to the cells. One of the first signs of this is called syncope, which is the same this as passing out and becoming unconscious because the brain does not get enough blood at the proper pressure.
Heart block– Occurs when the electrical impulse has difficulty passing through the AV node. There are 3 different degrees of heart block- 1st, 2nd, and 3rd.
Atrial fibrillation – When the atria contract in an irregular way and blood does not flow out of them effectively. This is initially detected during an exam with the stethoscope as a pulse deficit. A pulse deficit is a difference between when the heartbeat is heard with the stethoscope and when the pulse is felt at the femur with your hand. They should be simultaneous, in a pulse deficit they are not. It is confirmed with an EKG (electrocardiogram).
Ventricular fibrillation – When the ventricles contract in an irregular and ineffective way, a condition which quickly leads to death unless corrected. This is a heart attack in people, and needs a defibrillator to correct the problem. People who have serious arrhythmias can sometimes have an artificial pacemaker implanted in their chest or abdomen. This battery powered device delivers a rhythmic electrical impulse to the heart on either a constant basis, or only when the heart’s natural pacemaker temporarily fails to sustain a normal beat.
You will learn more about the SA node and AV node in the electrocardiogram section to follow, so try to keep their jobs in mind.
Graphic Photos On This Page
Thoracic Anatomy (heart, lungs, blood vessels)
The normal mammalian heart has 4 chambers (birds also have 4, reptiles have 3). The 2 smaller chambers are called atria, the larger ones are called ventricles. The diagrams at the beginning of this page described the flow of blood through these chambers. Now lets see what these chambers and valves actually look like. Click here to review the diagrams at the beginning of the page if you need to.
The following are necropsy (the same as an autopsy in people) pictures showing how these structures actually look. They are done tastefully and should not bother you. It will be obvious from these pictures that the real anatomy is much more complicated than the diagram pictures. We will be emphasizing the left ventricle and mitral valve, since that is the area of the heart that causes most of the problem as dogs age. We will trace the flow of blood from the left atrium, through the mitral valve, and into the left ventricle.
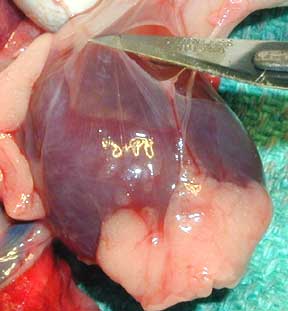
Before we even get to the heart, there is a layer called the pericardium that surrounds it. In some diseases, fluid can buildup in between this outer layer and the actual heart muscle. This is the pericardium from a normal ferret. The fat at the bottom of this heart is normal.
This picture shows mostly the inside of the left ventricle of a dog (its the same heart you saw at the very beginning of our heart page). You are looking into the chamber of the left ventricle. Note the thickness of the cardiac muscle (myocardium) surrounding the left ventricle, along with the smooth inner lining of the ventricle in the lower center of the picture. The lining needs to be smooth and relatively friction free for the red blood cells to flow through rapidly and not get ruptured or start clotting.

The tip of the metal hemostat (see arrow) just barely poking out is coming from the left atrium (not visualized), through the mitral valve, and barely into the left ventricle. This is the normal direction of blood flow as it comes out of the left atrium and into the left ventricle.
Let’s take a little closer look at the mitral valve. We have moved the hemostat a little further through the mitral valve in this next picture. Again, the left atrium is not visualized. The white filamentous structures are called chordae tendinae. When the blood flows through the mitral valve these chordae tendinae are relaxed since there is no pressure on them.
When the left ventricle contracts it exerts great pressure to get the blood through the aorta and to the rest of the body. This pressure pushes against the mitral valve, which is now shut since we do not want blood flowing backwards into the left atrium. It is these chordae tendinae that keep the mitral valve closed. A normal mitral valve can withstand this pressure, a diseased one cannot.

It is these strong chordae tendinae that prevent the blood from flowing back through the mitral valve into the left atrium. Remember this when we talk about mitral valve murmurs.
As we get even closer in the next picture you can see the leaflets of the mitral valve clearly (we removed the hemostat so you can see the bottom of the valve now). This thickened leaflet is called endocardiosis (you will learn more about this in the disease section when we teach you about chronic atrioventricular valve disease).
This thickening does not allow the valve to close fully, and blood regurgitates backwards into the left atrium when the left ventricle contracts. Since there is a huge difference in pressure (called a pressure gradient) between the left atrium and the left ventricle, this can have serious consequences.
This regurgitating blood is turbulent, and is the source of the heart murmur we hear with this disease. If the leakage is significant the pressure will cause the left atrium to enlarge (can be seen on a radiograph), with the potential for this added pressure to impede the flow of blood from the pulmonary vein.
If the blood in the pulmonary vein has a hard time flowing against this pressure in the left atrium, the plasma contained in the pulmonary veins will leak out of the capillaries and fill the lungs (the alveoli) with fluid. This is also called pulmonary edema, and is the “congestive” in congestive heart failure. Try to remember this when we discuss this in more detail later since it is an important aspect of chronic atrioventricular valve disease and congestive heart failure.

The top arrow points to a normal leaflet, the bottom arrow points to a thickened and shrunken leaflet
There are many other structures inside the chest (thorax) in addition to the heart and lungs. This next necropsy picture is from a dog. Before we show you the necropsy picture let’s get oriented using a chest radiograph.
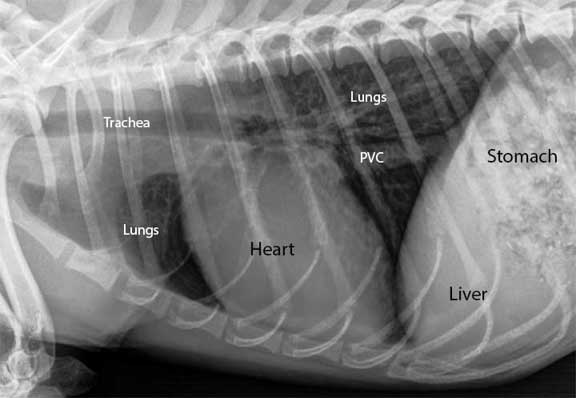
The dog is laying on its right side and the head is towards the left. This is the section of the thorax we will be looking at in the necropsy pictures to follow.
On the far right is the diaphragm (D), the muscle of respiration. It separates the thorax to the left of the diaphragm, from the abdomen on the right (the liver and stomach are just behind the diaphragm). The posterior vena cava (PVC) is visible as the horizontal blue structure at the bottom of the picture that is coming through the diaphragm. It is large because it has the job of returning almost all of the blood from the back end of the body to the heart.
The large horizontal pink structure above the posterior vena cava is the esophagus (E) as it goes through the diaphragm and enters the stomach behind the diaphragm on the right. It is not visible on the X-Ray above.
You can see one of the posterior lung lobes above and to the left of the esophagus. If you look closely you can also see a white nerve running horizontally along the esophagus (vertical arrow).
If you look even closer you can see a large white structure running horizontally just above the esophagus (horizontal arrow)- its the aorta embedded in tissue for protection.

With all of this anatomy packed into the thorax its a wonder we can even breathe at all!
The next picture is the same picture as the previous one, only viewed from the top and not the side. The head is towards the top with the dog laying on its back, the diaphragm (D) is at the very bottom. The structures are labeled the same.
Notice how much more lung is visualized. Look at the large veins to the lung lobes in the upper right. The posterior vena cava (PVC) is obvious as it runs vertically exiting the diaphragm at the very bottom of the picture and enters the right atrium at the top of the picture.
On each side of the vena cava are pink lung lobes, then the red esophagus (E), then the white aorta (A). Keep in mind these lungs are deflated. Think of how crammed this space is when the lungs are filled with air as we inhale. As a matter of fact, the negative and positive thoracic pressures that occur when we breathe have an influence on how this blood flows.

When normally inflated the lungs will fill the remainder of the thoracic cavity
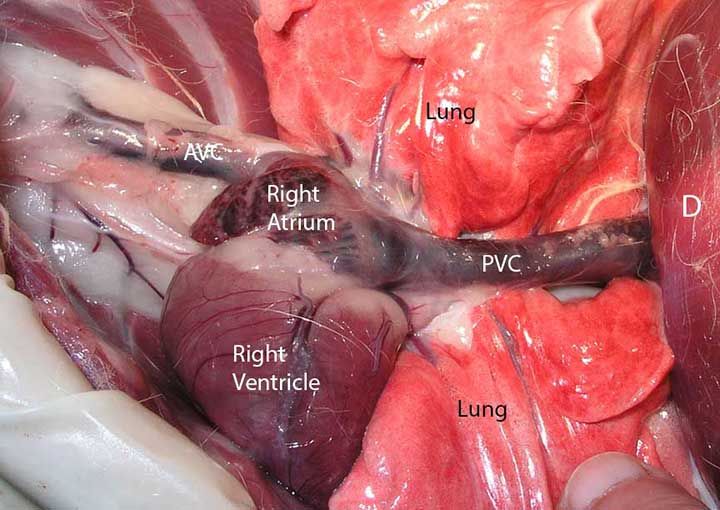
In the next side view picture we are shifted towards the left and away from the diaphragm and going closer to the heart. The head is still at the left. The heart is the dark blue structure on the top. The pericardium (lining of the heart) is still around the heart, so the heart is not as apparent as you might expect.
The right atrium cannot be visualized because the heart is covered with the pericardium. You can see the posterior vena cava (PVC) on the right as it enters the right atrium. The PVC returns venous blood from the back of the body to the heart.

You can also see the anterior vena cava (AVC) on the left as it also enters the right atrium. The AVC returns venous blood from the head and neck to the heart. You can also see a nerve as it runs horizontally on top of each vena cava.
Here is the feline version of the same area. In the first picture we are looking at the right side of the heart. The structures are smaller, but being a mammal, the anatomy is the same.
You cannot see the aorta in this view because the lung lobes are covering it

In this picture we have lilted up the heart and rotated it to the right, so now we can see the left side of the heart and underlying structures like the aorta (A)
The walls of the aorta are much thicker that the pulmonary artery due to the added pressure of the blood as it is pumped out of the left ventricle. The pressure of the blood coming out of the right ventricle and going into the pulmonary artery is much less than the aorta, so the walls are not as thick

The opening to the pulmonary artery is on the left, the aorta opening is on the right.
Cardiac Physiology Overview
The cardiovascular system of the body is truly a miracle. This series of pumps and pipes literally is able to supply the billions of cells in the body with all their essential needs, and it does this in an environment of constantly changing needs.
A normally functioning heart needs to be working in optimum condition, able to instantly adjust to the varying needs of the body. For this to happen everything needs to work in unison:
The blood vessels to the heart need to be functioning normally. A problem here (atherosclerosis) is a disease seen usually in humanoids, not animals. When these blood vessels do not supply the heart with an adequate blood flow, a myocardial infarct (MI) occurs. This means that a section of heart muscle dies because of a lack of blood supply. This can lead to a heart attack in people.
The electrical conduction system has to be working in a coordinated fashion for the blood to flow efficiently through the heart chambers. If the problem is severe enough a heart attack can occur. In this condition the heart needs an external electrical charge (defibrillator) to shock it back into normal rhythm.
All of the heart valves need to be working optimally so that blood can flow in the proper direction and in adequate amounts. A leaking valve causes regurgitation of blood backwards into the wrong chamber. This abnormal blood flow leads to turbulence, which is picked up by the stethoscope as a murmur. If severe enough the problem can lead to congestive heart failure.
The heart chambers and muscles need to be the proper size for optimal flow of blood. Also, the septum that separates the right heart from the left heart needs to be intact. If not, blood can now flow directly from one ventricle to another, bypassing its normal route through the lungs.
A dilated heart chamber leads to dilated cardiomyopathy, which is a heart muscle too weak to beat with enough force to supply the cells with blood. A heart chamber that is too muscular, called hypertrophic cardiomyopathy, leads to a ventricle chamber size that is too small to fill up with enough blood for the body’s needs.
The arterial and venous systems need to be able to constrict and dilate so that proper blood pressure is maintained and also so all of the cells of the body get an adequate blood flow.
Cardiac Physiology
So far we have been easy on you. You need to put your thinking cap on for the next two sections on physiology and pathophysiology. We will try to make this as painless as possible by repeating important concepts, and doing it from a different point of view, or using a different example.
You might even want to read the next sections more than once, since they are the basis for the symptoms and treatment of congestive heart failure (CHF). Lets give it a try….
Before we get into the details of how it all works in a normal heart and a failing heart, let’s expose ourselves to some additional medical terminology. We will repeat this terminology several times in our discussion of physiology and pathophysiology.
cardiac output – the amount of blood in cc’s the heart pumps through the body each minute.
heart rate – the number of times the heart beats each minute
end diastole – the amount of blood left in the heart chambers after the heart’s relaxation phase (diastole)
preload – the amount of blood in the heart chamber that is left over from the previous contraction (end diastole), plus the amount of blood brought into the heart chamber from the venous system (the vena cava’s)
perfusion – adequate blood flow to a target organ (liver for example) and its multitude of cells
diastole – when the heart rests in between contractions
hypertension – high blood pressure
stroke volume – the amount of blood pumped out of the heart with each individual beat of the heart.
contractility – refers to the inherent strength of the myocardium to contract and pump blood
myocardial oxygen consumption (MVO2)– the amount of oxygen required by the heart muscle for a contraction
afterload – refers to the resistance the left ventricle encounters as it tries to eject blood to the body
systole – when the heart contracts
venous return – the blood brought into the heart from the venous blood supply
The whole point of the cardiovascular system is to provide the individual cells in each organ an adequate flow of blood (called perfusion) that gives them the nutrients and oxygen they need. When these cells have what they need they can perform their normal function.
So for the kidneys, that means they can filter out waste products. For the muscles, that means they can initiate movement. For the liver, that means that liver cells can metabolize drugs we put into the body. This adequate perfusion equates back to how much fluid the heart can deliver to these cells. An adequate cardiac output is needed for this perfusion.
Cardiac output is the amount of blood in cc’s pumped by the heart each minute. The determinants of cardiac output are the heart rate (measured in beats per minute) and the stroke volume (the amount of blood in cc’s ejected with each beat of the heart).
The ability of the heart to increase cardiac output is a very good thing. When you run a long distance, your muscle cells need more fuel than when they are at rest. The heart rate increases, along with the amount of blood ejected with each beat of the heart (increased heart rate and stroke volume).
This increases the perfusion to the muscle cells, and they now get more oxygen, glucose, and electrolytes. The increased perfusion also allows them to rid themselves of carbon dioxide and other waste products like lactic acid. The final outcome is muscles that operate faster and stronger.
Several factors affect cardiac output:
Preload
Afterload
Contractility- The strength of each contraction of the heart muscle
Heart rate- the number of times the heart beats each minute
Distensibility- the ability of the heart muscle to stretch and return to normal
Synergy of contraction- the normal coordinated beating pattern of the heart.
To keep it more understandable we will only discuss preload and afterload in the next sections.
Preload (end diastolic volume)
This is the priming process of the pump, and for practical purposes, consists mostly of the blood that the veins bring into the right and left atriums (atria). It occurs for that fraction of a second when the heart is not beating, which you know is called diastole. We also call preload end diastolic volume because it is the volume of blood in the heart chamber at the very end of diastole (just before systole starts). Technically, preload is equal to venous return plus the residual volume left in the cardiac chamber after the last contraction.
An increase in preload increases stroke volume. This is good to a point. It means that an adequate amount of blood is coming from the posterior vena cava and anterior vena cava to supply the right heart with the amount of blood it needs. It also means an adequate amount of blood is coming from the lungs (pulmonary veins) to supply the left heart with the amount of oxygenated blood it needs to supply the body.
At a normal resting state your preload is consistent. If you start exercising you need to bring more blood to the muscles for their needs. The venous system will bring more blood into the heart chambers during diastole (preload) so that the heart can eject more blood with each beat (increased stroke volume). In addition, the heart will beat faster (increased heart rate). The increased stroke volume and heart rate will increase cardiac output as per the formula above.
An increase in preload also increases afterload as the volume of the chamber increases. So, now let’s talk about afterload.
Afterload
Afterload refers to the resistance the left ventricle encounters as it tries to eject blood into the aorta when it contracts. It also refers to the resistance the right ventricle encounters as it ejects blood into the lungs to get a fresh supply of oxygen. We will come back to this later, for now, think of it as how hard the heart has to pump against the pressure in the aorta to get the blood moving along to all of the cells in the body.
Vascular resistance is how constricted or dilated an artery is as the blood is flowing through it. It is synonymous with blood pressure for our discussion. You already know that arteries constantly constrict and dilate, all depending on the needs of the body overall, and the specific organ they are supplying with blood.
Going back to our muscle scenario above, in addition to an increased cardiac output, the cardiovascular system also opens up (dilates) the arteries to the the muscles, which also adds to their perfusion. This blood pressure concept is very important, we need to cover it in more detail.
Normal regulation of the blood pressure involves a complicated set of metabolic processes. Many body systems are involved, including the nervous system, the renal system, the cardiovascular system, and the endocrine system. It is a highly refined system that can make minute changes in rapid response to changing physiologic needs.
There is a part of our brain and spinal cord that constantly monitors normal physiologic process that are going on in the body. It performs a myriad of functions, many of them crucial to our survival, that we are not even aware of. The part of our brain and spinal cord that does this is called the autonomic nervous system (ANS).
It is the ANS that continuously monitors blood flow and blood pressure. It does this through pressure monitoring structures called baroreceptors located near important blood vessels.
When the ANS detects a decrease in blood pressure, it activates a sophisticated set of physiologic processes to maintain adequate blood pressure, and thus adequate perfusion to critical organs like the brain and heart. The ANS tells the juxtaglomerular apparatus in the kidneys to secrete renin into the bloodstream. Renin converts the compound angiotensin to angiotensin I.
Angiotensin I circulates to the lungs, where an enzyme called angiotensin converting enzyme (ACE) converts it into angiotensin II, leading to significantly increased constriction of the blood vessels of the body in general. Angiotensin II also increases secretion of the hormone aldosterone from the adrenal glands, which further increases arterial constriction (increasing afterload), and increases venous constriction (increasing preload), and increase sodium and water retention (also increases preload).
The end result is the constriction or narrowing of many blood vessels to non-critical organs, which increases the blood pressure to the critical organs like the heart and brain.
Garden Hose analogy
As an analogy, consider the spigot as your heart, and the hose as the blood vessels that supply your lawn with water. Consider your lawn an organ like the liver, and each individual blade of grass as a liver cell.
If you turn on your garden hose only slightly there is a low pressure (low blood pressure) in the hose, and you can’t water very much of your lawn. Each blade of grass does not get enough water, so there is inadequate perfusion.
If you turn up the spigot all the way you increase the stroke volume leading to an increase in cardiac output. This increases the pressure (increased blood pressure) in the hose, and all the blades of grass will get enough water (better perfusion). The spigot is the cardiac output, the flow through the garden hose is the blood pressure, the amount of water each blade of grass gets is the perfusion.
In our hose analogy, preload is how much water the city is supplying to your spigot (the water company is the venous system bringing blood back to the heart).
Afterload is equivalent to how much force is needed by the spigot to get an adequate amount of water to the lawn (adequate perfusion). If you change hoses and hook up one that is smaller in diameter (increased vascular resistance) more force is needed from the spigot (more afterload) to give the lawn enough water (adequate perfusion).
This means the spigot has to do more work. If the spigot is the heart, this means that it has to contract harder to get that blood out to all those cells in the body. A healthy heart is up to this challenge, a diseased heart is not.
So now let’s see what happens when all of this complicated physiology has a problem, a process we call pathophysiology.
Pathophysiology of Heart Disease
There is a difference between heart disease and heart failure. In heart disease the heart has some type of abnormality. If minor enough, the heart is able to deliver adequate perfusion to the cells, and there is no problem, at least initially. An example might be a murmur that is not causing any problems.
In heart failure, the heart does not maintain an adequate perfusion for normal cell function. Pets that are relatively inactive may be able to stave off the effects of heart failure longer than active pets because they do not challenge the cardiovascular system. This has a bad side though, because by the time the symptoms of heart failure are finally apparent to an owner, the disease is well entrenched and more difficult to treat.
When the heart starts failing (decreased cardiac output) it is due to either a 1) decrease in stroke volume or 2) an abnormal heart rate:
1. Stroke volume may decrease secondary to reductions in preload (shock, dehydration, hemorrhage), poor contractility (cardiomyopathy), increased afterload, or inadequate heart valve function (endocardiosis, patent ductus arteriosis), or fluid around the heart (tamponade).
2. Abnormal heart rates are called arrhythmia’s, and are due to a problem with the electrical conduction system in the heart. A slow heart rate (bradycardia) will decrease cardiac output per the formula you have already been exposed to earlier. High heart rates (tachycardia) will increase cardiac output initially. As the heart rate continues to increase, at a certain point, it will decrease cardiac output because there is not enough time for the heart chambers to fill with blood during diastole. As a result, during systole when the heart is ejecting blood into the aorta, it ejects less blood with each beat.
In either case, heart failure is usually the culmination of a chronic process. This gives the body time to adapt to the small amount of inadequate perfusion in the beginning stages of heart failure. Compensatory mechanisms are initiated to increase the perfusion of the cells.
Initially, these compensatory changes work quite well. So well in fact, that you do not notice the early signs of heart failure in your pet. As time goes on though, the heart continues to fail further, and these compensatory changes no longer work. As a matter of fact, they eventually become detrimental. It is at this point in time that you start noticing the symptoms of heart failure.
From the bodies point of view, the inadequate perfusion of the cells during heart failure mimics what occurs when a healthy animal loses significant amount of blood or goes into shock. Shock is the collapse of the cardiovascular system, leading to significantly decreased perfusion of the cells. It can lead to death if not treated rapidly. A good example of shock is when a pet gets hit by a car.
A number of compensatory measures are built into the makeup of animals with the objective of rescuing the circulatory system in conditions of circulatory collapse or shock. There is inadequate circulatory volume (preload) to maintain cardiac output. Hence the body activates these compensatory measures to raise a depressed blood pressure (through increased vascular resistance) and increase a depressed cardiac output (through increasing contractility, increasing heart rate, and increasing preload) to maintain perfusion to the vital organs (brain and heart).
Although these measures may work adequately for the short term correction of shock, they are counterproductive when the state of shock lasts for more than several weeks, which is exactly what occurs in heart disease. Unfortunately, the body handles all situations that cause a decrease in cardiac output as a condition similar to shock, even if it is heart failure, and not shock, that is causing the poor perfusion to the cells.
Let’s look at these compensatory measures and how they contribute to the cascading series of events that leads a failing heart to congestive heart failure (CHF).
A failing heart leads to a decreased cardiac output. The body responds initially by increasing the heart rate and contractility (stroke volume), and thus the cardiac output, leading to increased cellular perfusion. The autonomic nervous system also constricts selective peripheral arteries, leading to an increased blood pressure to vital organs, and again, more perfusion to their cells.
This increased blood pressure increases afterload, putting further stress on a failing heart as it attempts to push the blood against more resistance. The autonomic nervous system also increases pressure in the venous system, which brings more blood back to the heart, increasing preload. You learned all about this in the physiology section, we are just reviewing it.
As the heart increases its contractility it also increases its demand for oxygen which can lead to an arrhythmia. If the arrhythmia is severe enough, the coordinated beating of the heart is diminished and a further reduction in cardiac output occurs. We monitor this with an electrocardiogram (EKG or ECG).
As the ANS redistributes blood flow it maintains cardiac output to the heart and brain (just like it does in shock) and away from peripheral vascular beds. It does this to keep the blood pressure at an adequate level. This shunting of blood to these vital internal organs and away from the other organs in the body eventually leads to pale mucous membranes, slow capillary refill time, and cool extremities.
As it progresses, blood is shunted away from the intestines, interfering with absorption of food. If severe enough, the intestines can become ulcerated and start hemorrhaging.
Blood is also shunted away from the kidneys, decreasing their efficiency by decreasing the glomerular filtration rate (GFR). This results in more sodium buildup and an increase in fluid retention, leading to a higher blood pressure and more preload and afterload. It also results in an increase in the amount of waste products that buildup in the bloodstream. You can find more information about these waste products in our kidney page.
As volume (preload) continues to increase, pressure in that heart chamber increases. If this occurs in the left heart, back pressure builds up in the pulmonary veins, which causes a leakage through the walls of these vessels and into the actual lung tissue (alveoli). The result is pulmonary edema, which is fluid buildup at the alveoli, the actual area where red blood cells exchange carbon dioxide and oxygen. This fluid will significantly interfere with this exchange. This is congestive heart failure.
As the heart tries to maintain adequate perfusion to the cells of the body, adequate perfusion of cells is useless if the red blood cells that supply these cells with oxygen do not have enough oxygen molecules in them to be of use to the cells.
Not only do we now have a heart that is not adequately perfusing the cells with oxygen and nutrients in general, we also have red blood cells that are having a hard time getting a fresh supply of oxygen because of the fluid buildup in the lungs. This double whammy affects all organs, even the heart itself. It is apparent that a vicious cycle develops from which the body cannot escape.

This white frothy fluid is severe pulmonary edema. It is a cut section of the lung of a cat that died from cardiomyopathy.
If the increased preload occurs in the right heart, the back pressure builds up in the veins that supply the the two atria. Since the posterior vena cava returns blood from the abdomen, an increased pressure here will cause the fluid to leak out of the vena cava and into the abdomen. This is called ascites. You will see what this looks like on a radiograph in our section on diagnosis heart disease.
Whether ascites or pulmonary edema occurs depends on whether this problem is occurring more in the left heart or the right heart. It can occur in both hearts, with the result of fluid buildup in several body cavities. Cats and dogs have different reactions to this also.
An increase in preload causes a marked increase in stroke volume for the normal heart, but only a modest increase in stroke volume for a failing left heart. So this compensatory mechanism has only a modest positive effect on cell perfusion. Conversely, reductions in preload cause a marked fall in stroke volume for the normal heart but only a modest reduction in stroke volume for the failing heart. Therefore, a marked reduction in preload in the heart failure setting will result in a resolution of pulmonary edema or ascites, with only a modest reduction in stroke volume.
This is of great clinical significance. Some of the drugs we use in a failing heart take advantage of their ability to lower preload without dramatically affecting stroke volume. The end result- the cells of the body get relatively adequate perfusion, while there is less pulmonary edema or ascites.
Even though the cells are not fully satisfied, the pet feels much better because there is less fluid buildup in the lungs and abdomen. Also, less fluid buildup in the lungs allows for proper oxygen and carbon dioxide exchange, which to say the least, is a critical physiological process.
We haven’t cured the problem with the drugs that reduce preload, but at least we make the pet feel much better, and allow for better oxygen exchange. This is huge for a pet or a person that is literally drowning in their own lung fluid.
The other compensatory change that occurs when perfusion of the cells is inadequate is an increase in afterload. This occurs as the body tries to raise the blood pressure to the critical organs like the heart and brain, which theoretically will give their cells more perfusion.
As was explained above, the body raises the blood pressure through several mechanisms. The already failing heart now has to pump against this increased pressure (more afterload), which decreases the stroke volume and further fatigues the heart. Changes in afterload have a more marked influence on stroke volume in the failing heart than the normal heart.
The ability to improve cardiac output by reducing afterload (blood pressure lowering medications) has been one of the major advances in cardiovascular therapeutics. We will talk about these medications in the treatment section. These are the exact same medications people use to lower their blood pressure.
Many other changes occur as the heart failure progresses. We already know that increases in heart rate cause an increase in cardiac output. This is great for cell perfusion but becomes self limiting when the heart rate increases to the point (180-250 beats per minute for the dog) that there is less time for the heart chambers to fill up with blood during diastole. This leads to an inadequate amount of blood pumped being out by the heart chambers during systole.
The increased heart rate also increases the oxygen consumption by the heart muscles, leading to an arrhythmia as they work harder and harder. Also, the heart is a muscle and needs proper perfusion to supply it with oxygen and nutrients just like all the other cells in the body. Blood flows into the heart only during diastole, and with the elevated heart rate, the heart spends less time in diastole. The end result is a failing heart that fails even faster because the myocardium (heart muscle) cannot get the blood it needs.
As the heart continues to fail the heart rate continues to increase and the heart muscle receives less and less perfusion. Eventually a point will be reached where the normal coordinated electrical beating of the heart can no longer function properly, and an arrhythmia occurs.
In this setting arrhythmia’s can dramatically reduce stroke volume and the heart failure can rapidly spiral out of control. It is at this point that the condition is critical, and usually when these pets are brought to us, often as a breathing emergency.
This cat is having a breathing emergency due to asthma, and is breathing in 100% oxygen. This is identical to the breathing problem encountered in heart disease.
A pet that cannot breathe well due to pulmonary edema (fluid in the lungs) is in a panic situation. It needs to be handled very gently, so the first thing we do is put it in 100% oxygen until it calms down. Only then do we attempt to diagnose and treat it.
Heart failure can also occur in conditions where the heart is producing a normal cardiac output, but the metabolic needs of the tissues are increased. Diseases such as feline hyperthyroidism or anemia fall into this category. Thus, heart failure can occur in conditions where the strength of the heart muscle appears normal, but the bodies need for perfusion is so great the healthy heart cannot keep up with the demand.
If the left heart becomes diseased it does not pump an adequate amount of blood (decreased cardiac output) through the aorta for distribution to the cells of the body. This inadequate flow of blood ((poor perfusion) prevents these cells from performing their normal functions The brain monitors this perfusion, and goes into action by regulating hormones and sodium in conjunction with the kidneys and the lungs.
This increases the pressure in the arterial system as a whole, and satisfies the needs of the cells temporarily by supplying them with a greater flow of blood (better perfusion). This added blood pressure fills the diseased left ventricle with blood more than usual (increased preload), causing it to dilate and weaken further. It also increases the pressure the left ventricle has to pump against (increased afterload) to get the blood through the aorta and into the cells.
These add further work to an already diseased heart, compounding the problem even further. Eventually, the blood presented to the left ventricle does not get pumped out effectively, which causes a back flow (added pressure) in the lungs. We will show this later radiographically by showing an enlargement of the left atrium.
When the pressure reaches a certain point the fluid in the blood vessels in the lungs leaks out, causing pulmonary edema. This is congestive heart failure (CHF), the pet that is not breathing well or coughing, and needs immediate treatment.
If the right heart becomes diseased, a similar set of physiologic sequences occurs. The higher blood pressure that results when the cells send their emergency signals to the brain results in a greater amount of blood being presented to the right heart (increased preload). Eventually, the weakened right heart cannot pump blood into the lungs faster than the venous system is presenting blood to it.
This causes back pressure to build up in the venous system, especially the vena cava and other veins in the abdomen and even thorax. When the pressure gets high enough in these veins fluid leaks out, leading to ascites and pulmonary effusion.
This problem can occur in both hearts at the same time, causing even more problems.
Pretty easy huh? Enough of this physiology and pathophysiology stuff, let’s move on to something a little easier…..